14 YEAR OLD FEMALE WITH FEVER
MEDICINE CASE DISCUSSION
14 YEAR OLD FEMALE WITH FEVER
- April 05, 2023
M. Anurag
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis
This is a case of a 14 year old girl who came with chief complaints of:
1. Cough since 7 days
2. Fever since 5 days, vomiting 5 days ago
3. Lower back ache since 1 month on and off
4. Pain during micturition
5. Generalised weakness and body pains
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 7 days ago, then she developed -
Cough insidious in onset and gradually progressive. Initially dry cough, later progressed to productive cough with no diurnal or seasonal variations.
Fever since 5 days, high grade associated with chills and rigours, relieved with medications, no aggravating factors.
Vomiting- 5 days ago of 2-3 episodes, with food as content.
Lower backache since 1 month. Generalised weakness and body pains are present.
Pain during micturition in the lower abdomen. No burning micturition. History of increased frequency of micturition.
Passing stools every 3 days. No history of weight loss.
PAST HISTORY:
History of similar complaints 2 years back , got admitted then.
In June 2021, she came with complaints of abdominal pain and vomiting for 6 days.
She was apparently asymptomatic 6 days back, later developed abdominal pain, sudden in onset, diffuse, dragging type, non radiating which relieves on rest, not aggravated on food intake.
Vomiting for 5 days, 2episodes/day, non projectile, non bilious, non blood stained, with food as content.
H/O decreased urine output for 6 days associated with burning micturition.
H/O loose stools for 2 days, 3-4 episodes/day, watery, yellowish, mucoid, non foul smelling
H/O fever for 2 days, relived on medication.
Child was admitted in PICU with above complaints and all necessary Investigations were done and was given symptomatic treatment with
INJ CEFOTAXIME
INJ PANTOP
INJ ZOFER
TAB SPOROLAC
SYRUP ZINCOVIT
-History of acute nephritis 4 years ago.
PERSONAL HISTORY
She is an 8th class student
Diet - mixed
Appetite - normal
Sleep - adequate
Bowel and bladder regular
Menarche not attained
FAMILY HISTORY
No significant family history
GENERAL EXAMINATION
Patient is conscious , coherent and cooperative. Well oriented to time place and person.
No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy, edema
VITALS:
Pulse - 98 bpm
BP - 120/80 mm Hg
RR - 18 cpm
Temp- 96.6 F
SpO2- 98% on room air


SYSTEMIC EXAMINATION:
RS: BAE ,NVBS, no added sounds
CVS : S1 ,S2 heard no murmurs
P/A : soft , non tender

CNS:
HIGHER MENTAL FUNCTIONS- INTACT
MEMORY- able to recognise her family members and recall recent events
SPEECH: normal
CRANIAL NERVE EXAMINATION- normal
REFLEXES-
RIGHT LEFT
BICEPS 3+ 3+
TRICEPS 2+ 2+
SUPINATOR 1+ 1+
KNEE 2+ 2+
ANKLE. 2+ 2+
SUPERFICIAL AND DEEP REFLEXES ARE PRESENT AND NORMAL
MUSCLE POWER-
RIGHT LEFT
UPPER LIMB
ELBOW 5/5 5/5
WRIST 5/5 5/5
HAND GRIP 5/5 5/5
LOWER LIMB
HIP 5/5 5/5
KNEE. 5/5 5/5
ANKLE 5/5 5/5
TONE- NORMAL IN UPPER AND LOWER LIMBS
NO INVOLUNTARY MOVEMENTS
SENSORY SYSTEM- ALL SENSATIONS ARE NORMAL
Referred to dermatology I/V/O itching all over the body, was diagnosed as scabies and adviced
1. PERMETHRIN 5% LOTION LA ON DAY1, DAY 8
2. Tab. TECZINE 5mg SOS.
INVESTIGATIONS:
Hemogram:
2/4/23
Hb-12.3gm/dl
TLC-5300cells/cu.mm
PLT- 3.95 lakhs/cu.mm
RBC- 4.45
3/4/23
Hb- 12.2gm/dl
TLC-7600 cells/cu.mm
PLT- 4.08 lakhs/cu.mm
RBC- 4.37
4/4/23
Hb- 12.5gm/dl
TLC- 6800 cells/cu.mm
PLT- 4.4 lakhs/cu.mm
RBC- 4.57
CUE:
Albumin- nil
Pus cells- 2-3
Epithelial cells- 2-3
MP strip test- negative
NS1 antigen- negative
WIDAL test- negative
Urine for C/S- No growth
Blood for C/S- No growth after 24hrs of aerobic incubation.
Sputum for C/S- Normal oropharyngeal flora grown.
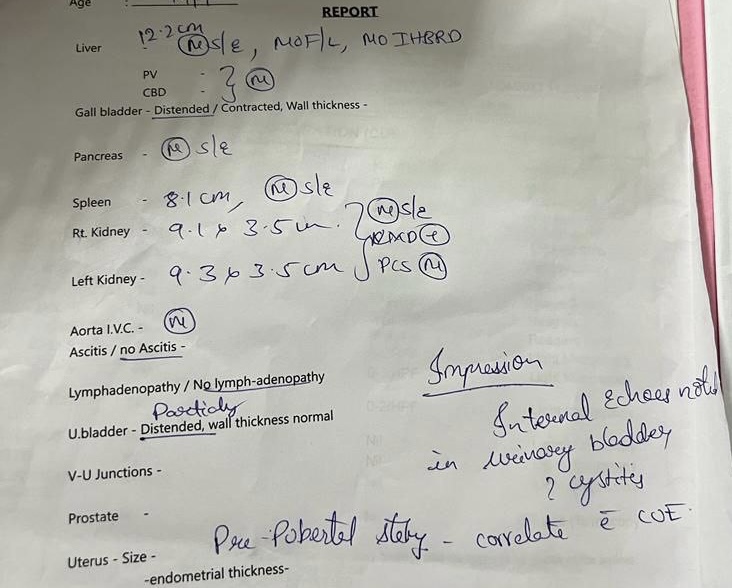


PROVISIONAL DIAGNOSIS:
VIRAL PYREXIA WITH CHRONIC CYSTITIS
TREATMENT:
1.TAB PCM 500mg PO/SOS
2. SYP ASCORIL LS PO/ TID
3. SYP CITRALKA 10ml PO/TID in 1 glass of water
4. PERMETHRIN 5% LOTION LA
5. TAB TECZINE 5mg PO/SOS


Comments
Post a Comment